

WHAT IS IT?
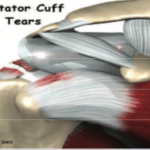
Figure 1
The supraspinatus tendon is the most susceptible to both traumatic injury and age-related attritional changes (see Figure 1). While traumatic injuries may occur in any age group, partial-thickness tears are usually seen in the fifth decade and full-thickness tears are frequently seen in the sixth and seventh decades of life.
HOW IS IT DIAGNOSED?
Pain and weakness generally lead to a rapid diagnosis after traumatic tears. A traumatic tears are less obvious, patients typically complain of a painful arc of motion and difficulty sleeping on the affected side. The pain often radiates along the course of the deltoid muscle into the upper arm. Mechanical symptoms of “clicking” and “catching” may also be present. Muscle testing may reveal variable degrees of weakness depending on the size of the tear. The Neer Impingement sign, Hawkins reinforcement test, and Jobe’s test may assist in diagnosing rotator cuff pathology. My preferred imaging modality is magnetic resonance imaging (the addition of gadolinium is usually not necessary except in the post-surgical shoulder).
HOW IS IT TREATED?
Restoration of shoulder function is most predictable for patients with an intact (healed) rotator cuff. Therefore, surgery is often recommended in the setting of acute rotator cuff tear, as well as the active, symptomatic patient. I will perform a minimally-invasive, all-arthroscopic repair in nearly 100% of patients who choose to have surgery (see Figures 2 and 3, before and after rotator cuff repair). Sedentary and elderly patients will often benefit from conservative measures including subacromial steroid injections, physical therapy, NSAIDS, and activity modification.
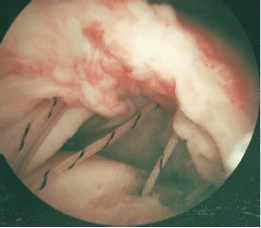
Figure 2
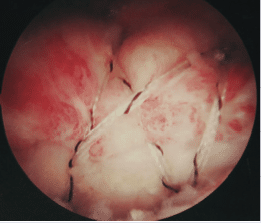
Figure 3
WHAT TO DO NEXT?
Because acute rotator cuff tears do better after timely repair, patients with traumatic shoulder pain and weakness require a more urgent diagnosis and possible referral to a shoulder specialist. Un-repaired rotator cuff tear size has been shown to increase over time. Smaller tears are easier to repair and have a higher chance of healing, and a lower re-tear rate. Conversely, larger tears are more difficult to repair and have a higher risk of re-tearing or incomplete healing. To put it simply, I prefer to repair small tears before they become big tears.