

The wrist is the link between the hand and arm and is responsible for positioning the hand in space so that it may perform the functions we expect. A complex set of bones and ligaments work together to achieve this important task. The complex anatomy of the wrist can make it challenging to accurately diagnosis wrist injury. Pain in the wrist can occur after injury from trauma, repetitive use, growths or masses, arthritis, or when nerves are trapped.
WRIST TRAUMA
A fall on the outstretched hand is the most common mechanism of wrist injury. When this happens, both bone and soft tissues structures in the wrist are vulnerable to injury (see Figure 1).
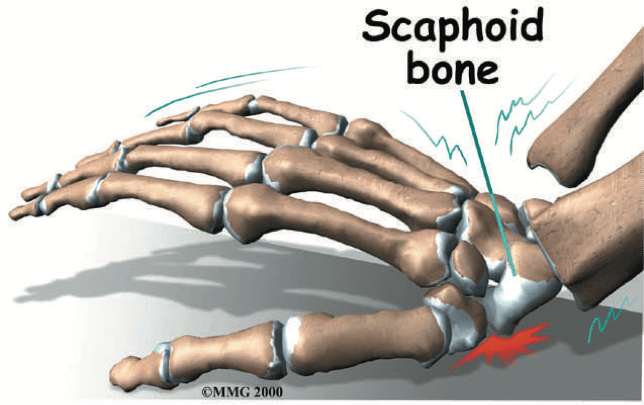
Figure 1
Bones: Fractures of the distal radius, scaphoid, and other carpal bones can occur. Plain radiographs are often sufficient to make the diagnosis, but because of the unique anatomy of the wrist, advanced imaging is often required. Carpal bone fractures, trabecular injury, and occult fractures can be seen on MRI.
Ligaments: Injury to the extrinsic ligaments of the wrist result in the common “wrist sprain,” but can be difficult to distinguish from injury to the intrinsic ligaments. Intrinsic ligament injury can be devastating and result in permanent wrist dysfunction if not properly diagnosed and treated. When plain radiographs do not show a fracture and there is persistent wrist pain, an MRI-arthrogram of the wrist can be helpful in establishing the diagnosis.
WRIST OVERUSE
Repeated use of the wrist for activity without adequate rest is a risk factor for developing wrist pain. The pain is commonly from tendonitis involving the tendons that cross the wrist.
Activities that can be troublesome are often work-related or avocational. Fortunately, with adequate rest, anti-inflammatory medicine, and directed hand therapy these conditions usually resolve. Directed hand therapy can be particularly helpful in identifying the offending activities and establishing proper ergonomics that eliminate the symptoms.
WRIST MASSES
Lumps and bumps occurring on or around the wrist can result in pain and dysfunction. Ganglion cysts are the most common masses found in the wrist (see Figure 2). They can arise from any joint in the wrist and do not require treatment unless they are symptomatic. Other masses that can occur in the hand include solid tumors (the overwhelming majority are benign) and tenosynovitis (swelling of the tendon linings). Clinical evaluation can provide the diagnosis with a high degree of certainty for characteristic masses. Advanced imaging has a role in establishing the diagnosis and aiding in preoperative planning.
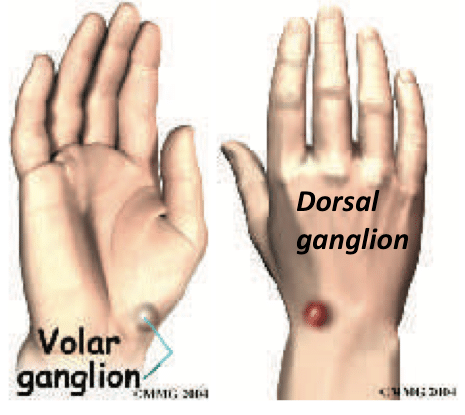
Figure 2
WRIST ARTHRITIS
Arthritis can affect any joint in the wrist (see Figure 3). Often the etiology is post-traumatic, either from fracture or prior ligament injury. Inflammatory arthritis can also be a cause of primary wrist arthritis. True “wear and tear” arthritis is less common.
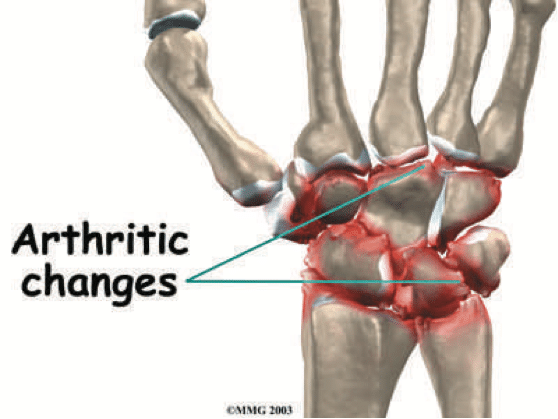
Figure 3
NERVE ENTRAPMENT
Wrist pain can also result when the nerves that supply the hand and wrist become “pinched.” The pinching can occur at the level of the wrist (carpal tunnel and guyon canal), elbow (cubital and radial tunnel), or up at the neck (disc herniation). Wrist pain that results from nerve entrapment can mimic other conditions. It often begins as a vague pain at the wrist with increased activity. Numbness will accompany the pain, but often the earliest signs will be pain associated with activity.
THE BOTTOM LINE
Treatment of wrist injury is dependent upon an accurate diagnosis. A thorough history and physical exam, together with plain film radiographs, will often suggest the correct diagnosis. Additional studies can be helpful to confirm the diagnosis when the risk of missing the diagnosis is significant.
Hand therapy is an important adjunct for treatment of wrist injury that helps with both rehabilitation, recovery, and prevention. It is important to work with a specialized Hand Therapist who is trained and focused on the hand and upper extremity.
WHAT TO DO ABOUT WRIST INJURY?
Trauma: Non-displaced fractures about the wrist can be treated with cast immobilization for 6 weeks (except for the scaphoid-12 weeks). Fractures involving the joint surfaces or with displacement often require surgery.
Tendonitis: Most tendonitis responds to rest, splinting, antiinflammatory medicine. Directed hand therapy helps with a focus on recovery and prevention.
Masses: Most masses about the wrist are benign and can be observed. For ganglion cysts, resting the wrist with a splint when symptomatic and steroid injections can be helpful. Tenosynovitis should be evaluated because its long-term presence can lead to erosion of the tendons and rupture.
Arthritis: Most wrist arthritis is treated with anti-inflammatory medicine, splinting, and activity modification. Steroid injections can be helpful on a periodic basis. Sometimes surgery is necessary but only after failure of all nonoperative treatments.
Nerve entrapment: Splinting to relieve pressure on the nerve, working with directed Hand Therapy, and careful attention to how the extremity is used can minimize the effects of nerve entrapment. Sometimes surgery is required to relieve pressure.